Evaluation of renal functions tests among Sudanese healthy pregnant women attending antenatal care (ANC) at The National Ribat University Hospital in Khartoum State in 2019
Renal function tests in Sudanese pregnant women
Revised : 2020-12-24
Accepted : 2020-12-26
Online : 2021-01-14
Print : 2021-01-15



Full text
Abstract
Pregnancy involves remarkable physiological changes and the functional impact of pregnancy on the kidney physiology is widespread involving practically all aspects of kidney functions. The aim of this study was to evaluate the renal functions in Sudanese healthy pregnant ladies during different trimesters. A cross sectional study was carried out during July to October 2019 on Sudanese healthy pregnant ladies attending antenatal care at the National Ribat University Hospital in Khartoum State. The study covered 60 healthy pregnant ladies (20 for each trimester). The purpose of the study was explained to all participants and they were assessed after taking their consent. Blood pressure (BP) and body mass index (BMI) were measured by standard techniques. A sample of five ml venous blood was taken in a suitable blood container for measurement of urea and creatinine using a fully automated Mindray BS-300 Chemistry Analyzer (Mindray Bio-Medical Electronics Co., Ltd., Shenzhen, China). The data was analyzed using SPSS version 25 (IBM SPSS Inc.,Chicago, IL, USA), t-test was used to compare the statistical significant (p value ≤ 0.05 was considered statistical significant). The mean age of participants was 26.6±5.3 years with the range of 18-37 years. The mean BMI was 25.7±3.6 with the range of 18-31. The mean urea in the first, second and third trimester was 13.4, 13.9 and 13.2 mg/dl respectively with no statistically significant variation. The mean creatinine in the first, second and third trimester was 0.6, 0.6 and 0.5 mg/dl respectively with no statistically significant variation. To conclude, there was no significant variation of serum urea and creatinine during three trimesters of pregnancy in healthy pregnant women.
Keywords: Creatinine, Pregnancy, Urea
How to cite: Ali IA, Hassan EB, Elhassan KS. Evaluation of renal functions tests among Sudanese healthy pregnant women attending antenatal care (ANC) at The National Ribat University Hospital in Khartoum State in 2019. Ann Med Physiol. 2020 Oct-Dec;4(4):24-28. doi: 10.23921/amp.2020v4i4.28248
Introduction
Pregnancy involves remarkable physiological changes and the functional impact of pregnancy on the kidney physiology is widespread involving practically all aspects of kidney functions and during the pregnancy the glomerular filtration rate (GFR) increases by 50% with subsequent decrease in serum creatinine, urea and uric acid levels. Also the threshold for thirst and antidiuretic hormone (ADH) secretion are depressed resulting in lower osmolality and serum sodium levels [1].
Some published literature evaluated the changes in renal functions in pregnancy. In 1984, South African study consisting of 94 pregnant women assessed the serum electrolytes and compared them with the levels in non-pregnant control matched for age and sex. The study was showed that the urea and creatinine decreased markedly throughout pregnancy [2].
Another study was performed using plasma iohexol to evaluate glomerular filtration rate in pregnancy and concluded that the glomerular filtration rate was elevated by 40% throughout pregnancy and during the first week of post partum period, and fell to levels similar to non-pregnant within one month [3].
In 2018, a meta-analysis of 49 studies from different sources, data synthesis included 4421 serum creatinine values in pregnancy, weighed according to cohort study, showed that the mean values for serum creatinine during the first, second and third trimesters of pregnancy were 84%, 77% and 80% of non-pregnant mean values respectively [4].
In 2000, a study used a large cohort of women experiencing normal pregnancy; modern laboratory technique and statistical analysis to construct across sectional interval. The study showed that the upper limit of normalcy for creatinine is higher than previously suggested and still lower than non pregnant values [5].
Among 12,41,286 pregnancies in Ontario during the study period; 2,43,534 (20%) were included in the final cohort study, there were 3,61,945 measurements of serum creatinine concentration among cohort with a median of one measurement per pregnancy, the mean serum creatinine concentration was 60 umol/l before pregnancy, rapidly decline by 4 weeks gestation to a nadir of 47 umol/l between 16 and 32 weeks, after 32 weeks gestation there was a steady increase in serum creatinine peaking at 64 umol/l within a few weeks postpartum and then gradual return to mean pregnancy concentration by 18 weeks postpartum [6].
In a study aimed to assess kidney function during normal pregnancy, the urea clearance test was run 93 times on 13 normal pregnant women from fifth month of pregnancy to eighth month postpartum, 10 times on 4 normal non pregnant women and before and after feeding urea to 7 pregnant women, the mean antepartum urea clearance was 153% of normal, this was significantly higher than the postpartum mean of 95.5% or than the mean of 105% for non-pregnant women, and there proportion between the low blood urea and high urea clearance of pregnancy and rising blood urea by feeding urea did not effect the high urea clearance [7].
Serial renal function studies have been carried out on 9 control subjects and 12 pregnant subjects from the fifteenth through the fortieth weeks of pregnancy and at intervals during the puerparium with the following result — the renal blood flow was 25% higher than control subjects throughout early and mid pregnancy then decline to control group during the last trimester and decrease below control for many months during the puerparium. The glomerular filtration rate increased by 50% throughout the pregnancy and return to non pregnant ranges early in the puerparium, the urea and creatinine concentration reduced approximately one half and two third respectively of non pregnant subjects [8].
An analytical study conducted during March to July 2012 compared plasma level of urea, creatinine, uric acid and albumin of 80 healthy pregnant women as a test group and 40 healthy non pregnant women as a control group to find if there are any changes in urea, creatinine, uric acid and albumin between the two groups. All the participants in this study were from Khartoum State, the study showed that the means of plasma level of urea and creatinine were less in the test group in all trimesters when compared to control group while uric acid and albumin was lower than control group but statistically not significant [9].
Tests of renal functions in pregnancy must be interpreted in relation to the changes in plasma volume, glomerular filtration and tubular reabsorption that normally occur with advancing gestation, blood urea nitrogen and serum creatinine levels are crude indices of renal function, the blood urea nitrogen normally decrease from non pregnant levels of 12 mg/dl to 9 mg/dl and plasma creatinine levels decrease from non pregnant mean value of 0.07 mg/dl to 0.05 mg/dl, if serum creatinine exceed the 0.08 mg/dl or blood urea nitrogen exceed the 14 mg/dl at any stages of pregnancy, renal dysfunction should be suspected [10].
The physiological increase in glomerular filtration rate in pregnancy normally results in a decrease in concentration of serum creatinine which falls by an average of 0.04 mg/dl to a pregnancy range of 0.04 mg/dl to 0.08 mg /dl, hence a serum creatinine of 1.0 mg/dl reflect renal impairment in pregnant women. The modification of diet in renal disease (MDRD) formula, which estimates a glomerular filtration rate using a combination of serum markers and clinical parameters have become a standard clinical method to estimate renal function in patients with chronic kidney diseases, the use of this formula has not been well studied in the pregnant population. Creatinine based formulas developed in non pregnant population are likely to be inaccurate when applied to pregnant women because the fall in serum creatinine during pregnancy reflects not only the pregnancy-induced increase in renal glomerular filtration rate but also hemodilution resulting from the 30 to 50% plasma volume expansion by pregnancy [11].
In Sudan, Abeadalla et al [12] established normal reference value of adults Sudanese for serum creatinine and urea in Khartoum State for healthy 444 subjects between 20 and 60 years. Their results showed that the reference range of serum creatinine and urea levels in in Sudanese non pregnant females were 0.76 mg/dl and 22.3 mg/dl respectively.
The objective of this study was to evaluate the renal functions in Sudanese healthy pregnant ladies during different trimesters and to examine the impact of pregnancy on it.
Materials and methods
A descriptive cross sectional study was carried out during July to October 2019 on Sudanese healthy pregnant ladies at the National Ribat University Hospital in Khartoum State. Ethical approval of this study was obtained from the National Ribat University Hospital. The study covered 60 pregnant women who agreed to participate in the study, 20 of them in each trimester. Women with history of hypertension, diabetic, pre-eclampsia, renal problem and who refused to participate in the study were excluded. Written consent was obtained from all participants after fully explaining to them the study purpose. An interview questionnaire was filled by all volunteers containing the data about name, age, address, medical history, drug use and lifestyle.
Blood pressure (BP), body weight and height were measured by standard techniques. Body mass index (BMI) was then calculated. All measurements were recorded in the data collection sheet.
About five ml venous blood sample was taken in the heparinized tube containers for measurements of urea and creatinine using a fully automated Mindray BS-300 Chemistry Analyzer (Mindray Bio-Medical Electronics Co., Ltd., Shenzhen, China).
The lab results was recorded in data sheet and compared with the normal laboratory range of the same gender.
Data analysis
Statistical analysis was performed using SPSS version 25.0 (IBM SPSS Inc.,Chicago, IL, USA). Proportions of the studied groups were expressed in percentages and means were used to describe the study variables. Independent sample t-test was used to compare between the three trimester groups. The p value ≤ 0.05 was considered significant.
Results
This cross sectional study was aimed at evaluating the renal functions in Sudanese healthy pregnant ladies in different trimesters. 60 pregnant women were involved in the study, distributed according to the trimester, 20 women in each trimester.
The mean age of the participants was 26.6±5.3 years with the range of 18-37 years. The mean body mass index (BMI) was 25.7±3.6 with the range of 18-31 (Table 1).
| Variable | Mean | Standard deviation | Maximum | Minimum | Range | Variance |
|---|---|---|---|---|---|---|
| Age (years) | 26.60 | 5.32 | 37 | 18 | 19 | 28.25 |
| Systolic BP (mm Hg) | 95.50 | 8.94 | 120 | 80 | 40 | 79.91 |
| Diastolic BP (mm Hg) | 63.33 | 9.94 | 80 | 40 | 40 | 98.82 |
| Weight (kg) | 61.68 | 9.82 | 76 | 40 | 36 | 96.39 |
| Height (cm) | 154.80 | 6.26 | 165 | 140 | 25 | 39.20 |
| BMI (kg/m2) | 25.79 | 3.69 | 31 | 18 | 13 | 13.60 |
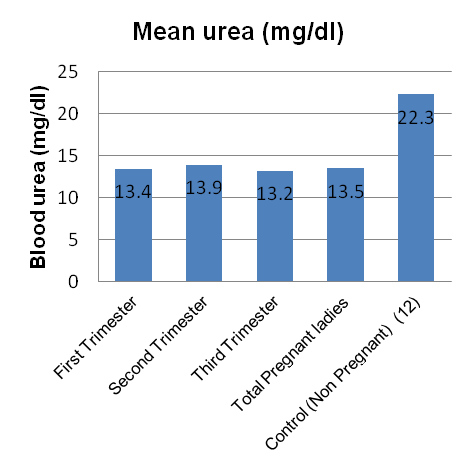
The mean urea in the first, second and third trimester was 13.4 mg/dl, 13.9 mg/dl and 13.2 mg/dl respectively with no statistically significant variation (Table 2) (Figure 1).
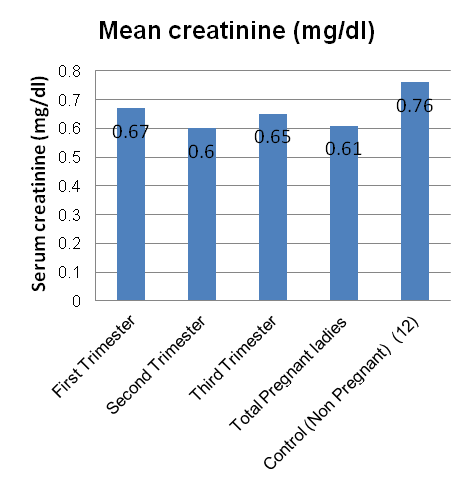
The mean creatinine in the first, second and third trimester was 0.6 mg/dl, 0.6 mg/dl and 0.5 mg/dl respectively with no statistically significant variation (Table 2) (Figure 2).
The mean urea and creatinine in the all pregnant women was 13.5±3.0 mg/dl and 0.6±0.1 mg/dl (Table 2).
| Test | Trimesters | N | Mean | Standard deviation | Minimum | Maximum | p value |
|---|---|---|---|---|---|---|---|
| Blood urea (mg/dl) | First | 20 | 13.40 | 2.22 | 10 | 16 | 0.876 |
| Second | 20 | 13.90 | 4.61 | 9 | 24 | ||
| Third | 20 | 13.20 | 1.75 | 10 | 16 | ||
| Total | 60 | 13.50 | 3.026 | 9 | 24 | ||
| Serum creatinine (mg/dl) | First | 20 | 0.67 | 0.09 | 0.50 | 0.80 | 0.134 |
| Second | 20 | 0.60 | 0.15 | 0.40 | 0.90 | ||
| Third | 20 | 0.56 | 0.11 | 0.40 | 0.76 | ||
| Total | 60 | 0.61 | 0.13 | 0.40 | 0.90 |
Discussion
This cross sectional study was aimed to evaluate the renal functions in Sudanese healthy pregnant women in different trimesters. A total of 60 healthy Sudanese pregnant women were recruited in the study. The distribution of study subjects was equal in each trimester (i.e. 20 women).
A previous study conducted by Abeadalla et al [12] established normal reference value of Sudanese adults for serum creatinine and urea in Khartoum State by testing 444 healthy subjects between 20 and 60 years. Their results showed that the reference range of serum creatinine and urea levels in Sudanese non pregnant females was 0.76 mg/dl and 22.3 mg/dl respectively.
In our study the blood urea ranged from 9 to 24 mg/dl which was lower than the normal range of non-pregnant ladies from 40% - 52% of the lower and upper limits respectively. The serum creatinine ranged from 0.4 to 0.9 mg/dl which was also lower from normal range to non-pregnant by 33% - 18% of the lower and upper limits respectively.
The findings of this study showed the mean urea and creatinine levels decreased in all trimesters of pregnancy when compared to the non-pregnant control group, which is in agreement to the study published by De Flamingh et al [2]. They found that the serum urea and creatinine decreases in all trimesters compared to non-pregnant group. Also the finding of this study was in agreement to the study by Elbashir et al [9] done in Sudanese healthy women at Khartoum State and concluded that the urea and creatinine levels decreased in all trimesters of pregnancy when compared to non-pregnant control group.
In our study the mean values of creatinine were 89%, 80%, 74% of the non-pregnant values in the first, second and third trimesters respectively which is comparable to the study published in March 2019 by Kidney International Reports were in the mean values of creatinine in pregnant women were 84%, 77% and 80% of the non-pregnant values during the first, second and third trimesters respectively [4].
Conclusion
The results of this study showed that the serum urea and creatinine decreases significantly in pregnant women in comparison to non-pregnant women. However, there was insignificant variation of serum urea and creatinine during three trimesters of pregnancy.
Availability of data and material
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
- Cheung KL, Lafayette RA. Renal physiology of pregnancy. Adv Chronic Kidney Dis. 2013 May;20(3):209-14. [Crossref] [Pubmed] [Pubmed Central]
- De Flamingh JP, van der Merwe JV. A serum biochemical profile of normal pregnancy. S Afr Med J. 1984 Apr 7;65(14):552-5. [Pubmed]
- Krutzén E, Olofsson P, Bäck SE, Nilsson-Ehle P. Glomerular filtration rate in pregnancy: a study in normal subjects and in patients with hypertension, preeclampsia and diabetes. Scand J Clin Lab Invest. 1992 Sep;52(5):387-92. [Crossref] [Pubmed]
- Wiles K, Bramham K, Seed PT, Nelson-Piercy C, Lightstone L, Chappell LC. Serum creatinine in pregnancy: A systematic review. Kidney Int Rep. 2018 Oct 29;4(3):408-419. [Crossref] [Pubmed] [Pubmed Central]
- Girling JC. Re-evaluation of plasma creatinine concentration in normal pregnancy. J Obstet Gynaecol. 2000 Mar;20(2):128-31. [Crossref] [Pubmed]
- Harel Z, McArthur E, Hladunewich M, Dirk JS, Wald R, Garg AX, Ray JG. Serum creatinine levels before, during, and after pregnancy. JAMA. 2019 Jan 15;321(2):205-7. [Crossref] [Pubmed] [Pubmed Central]
- Nice M. Kidney function during normal pregnancy I. The increased urea clearance of normal pregnancy. J Clin Invest. 1935 Sep;14(5):575-8. [Crossref] [Pubmed] [Pubmed Central]
- Sims EA, Krantz KE. Serial studies of renal function during pregnancy and the puerperium in normal women. J Clin Invest. 1958 Dec;37(12):1764-74. [Crossref] [Pubmed] [Pubmed Central]
- Elbashir SM. Assessment of renal function during various trimesters of pregnancy in healthy Sudanese women [dissertation]. Khartoum: Sudan University of Science and Technology 2012. Available from: http://repository.sustech.edu/handle/123456789/1556
- Hnat, M, Sibai B. Renal disease and pregnancy. Glob Libr Women's Med. 2008. [Crossref]
- Maynard SE, Thadhani R. Pregnancy and the kidney. J Am Soc Nephrol. 2009 Jan;20(1):14-22. [Crossref] [Pubmed]
- Abeadalla AA, Bashir AA, Abdalla IM, Ali IA, Awad KM, Mohmed AA, Musa OA. Normal reference value of adult Sudanese serum creatinine and urea in Khartoum state. Int J Health Sci Res. 2018; 8(6):19-24. Available from: https://www.ijhsr.org/IJHSR_Vol.8_Issue.6_June2018/IJHSR_Abstract.04.html